Brief Summary
This tutorial explores the shoulder joint from a lateral view, detailing its bony structures, joint cavity features, ligaments, muscles, and bursae. It covers the glenohumeral joint, scapula, and humerus, explaining how these components contribute to the joint's stability and movement. The video also touches on clinical correlations such as subacromial bursitis and painful arc syndrome.
- Overview of the shoulder joint's anatomy from a lateral perspective.
- Explanation of the bones, ligaments, muscles, and bursae involved in the joint.
- Discussion of clinical conditions related to the shoulder joint.
Introduction
The tutorial introduces an exploration of the shoulder joint from a lateral view, which provides a unique perspective for understanding the interaction and relationships of muscles from the anterior and posterior sides. The aim is to help viewers answer questions about the shoulder joint on anatomy exams. The tutorial will cover the shoulder joint, its bones, the joint cavity, ligaments, muscles, and bursae, as well as clinical notes.
Shoulder Joint Overview
The shoulder joint, or glenohumeral joint, is a ball and socket synovial joint in the proximal upper limb, allowing for a wide range of movements including flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction. It is the most mobile joint in the body, formed by the humerus and scapula. The head of the humerus articulates with the glenoid cavity of the scapula. Key features of the humerus include the lesser and greater tubercles and the inter-tubercular groove, which serve as attachment sites for structures that stabilize the joint. The scapula's relevant structures include the glenoid cavity, supraglenoid tubercle, infraglenoid tubercle, acromion process, and coracoid process, all crucial for muscle and ligament attachments that support the shoulder joint.
The Joint Cavity
The glenoid cavity, or glenoid fossa, forms the socket part of the shoulder joint, but it is shallow and has a small contact area with the humeral head, which impacts stability. The glenoid labrum, a fibrocartilaginous ring around the glenoid fossa, deepens the socket to improve stability. The joint capsule, made of a fibrous layer and a synovial membrane, surrounds the glenohumeral joint and secretes synovial fluid for lubrication. The fibrous part of the capsule engulfs the humeral head, extending to the anatomical neck of the humerus, forming the osteofibrous acetabulum with the glenoid cavity.
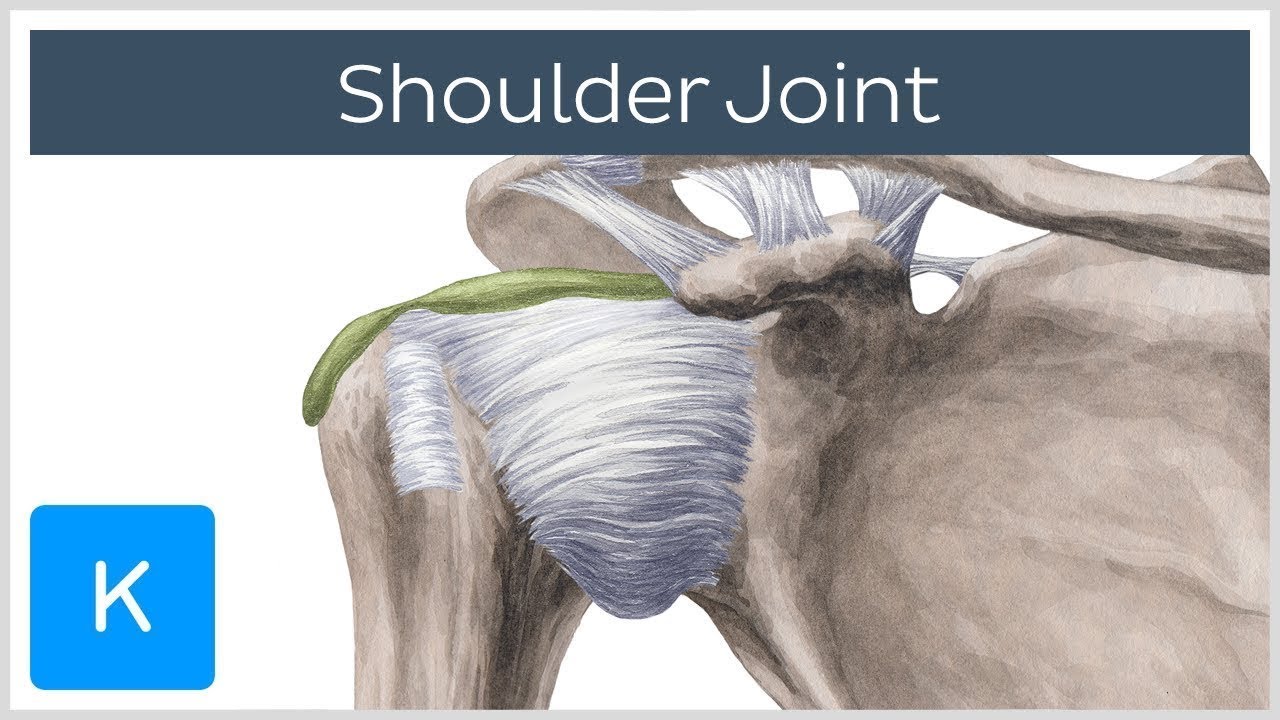
Ligaments of the Shoulder Joint
The joint capsule is strengthened by ligaments, including the coracohumeral ligament, which runs from the coracoid process to the humerus, preventing inferior displacement. The glenohumeral ligaments consist of the superior, middle, and inferior ligaments. The superior glenohumeral ligament spans from the supraglenoid tubercle to the inter-tubercular groove, working with the coracohumeral ligament to prevent inferior displacement. The middle glenohumeral ligament, located on the anterior aspect, originates inferior to the superior ligament and inserts on the lesser tubercle, adding anterior stability. The inferior glenohumeral ligament runs across the inferior aspect, originating along the glenoid margin and attaching to the neck of the humerus. All these ligaments blend with the capsule. The coracoacromial ligament, separate from the joint capsule, runs from the coracoid process to the acromion process, forming a superior arch above the humerus.
Muscles Supporting the Shoulder Joint
The rotator cuff muscles—supraspinatus, infraspinatus, teres minor, and subscapularis—create a compressive force around the humeral head, ensuring stability against the glenoid cavity. The supraspinatus originates from the supraspinous fossa and inserts on the greater tubercle, blending with the joint capsule. The infraspinatus originates from the infraspinous fossa and also inserts on the greater tubercle, strengthening the joint posteriorly. The teres minor originates from the lateral border of the scapula and inserts on the greater tubercle. The subscapularis, located on the anterior aspect, originates from the subscapular fossa and inserts on the lesser tubercle. Other muscles contributing to stability include the teres major, which originates from the inferior angle of the scapula and inserts on the intertubercular groove, and the long head of the triceps brachii, which originates from the infraglenoid tubercle. The long head of the biceps brachii originates from the supraglenoid tubercle within the joint capsule and travels through the inter-tubercular groove.
Bursae of the Shoulder Joint
Bursae are sac-like structures that act as cushions within the joint space. The subacromial bursa, the largest in the glenohumeral joint, lies deep to the coracoacromial ligament and acromion process, creating padding between these structures and the supraspinatus tendon. It extends laterally to become the subdeltoid bursa, reducing friction and preventing wear of the supraspinatus tendon during abduction. This bursa does not typically communicate with the joint capsule. The subtendinous bursa of the subscapularis, located on the anterior aspect, sits beneath the subscapularis tendon to reduce friction and prevent wear. Unlike the subacromial bursa, it usually connects to the glenohumeral joint.
Clinical Correlation: Subacromial Bursitis
The subacromial bursa can become inflamed, causing subacromial bursitis, often due to overuse or trauma. This inflammation is aggravated during shoulder abduction and can cause pain when lying on the affected shoulder. Damage to structures under the acromion process, such as the subacromial bursa and supraspinatus tendon, can result in painful arc syndrome, characterized by pain during arm abduction between 60 and 120 degrees.
Review
The tutorial reviews the features of the joint cavity, including the glenoid cavity and labrum, and the glenohumeral capsule. It revisits the ligaments such as the coracohumeral, superior, middle, and inferior glenohumeral, and the coracoacromial ligaments. The review also covers the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis), teres major, long head of the triceps brachii, and long head of the biceps brachii. Finally, it summarizes the subacromial and subtendinous bursae and the clinical implications of subacromial bursitis and painful arc syndrome.

